
We always think of Nephrotic Syndrome- >3gm of protein loss. Where did that come from? What is the evidence? Why not 2gm and why not 4gm? A nice post from Nephrohug( in French) discusses this topic in detail.
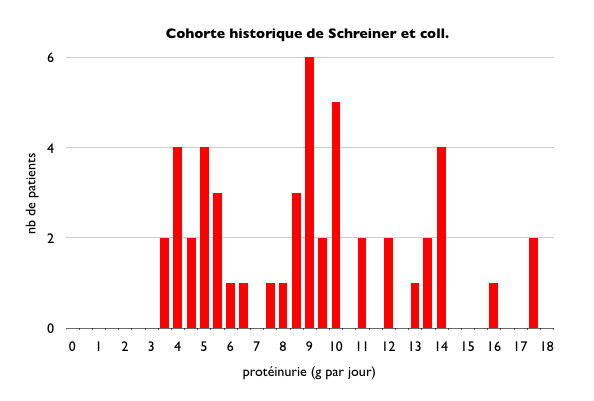
It dates as early as 1960s that Dr. Schreiner described in a paper called Glomerular Permeability in the Nephrotic Syndrome. In that paper, lot has been described but interestingly there is a Figure 4 that( look at first ref below) that shows 184 patients with glomerular diseases and most >3.5gm were considered nephrotic range and had a different pathology compared to <3.5gm. But the range is 2.5-3.5gm. He noted that the clinical parameters ( albumin, lipids, exam) were different in the >3.5 group. The author notes that the garden variety diseases like pyelonephritis, benign nephroscloerosis, certain lupus nephritis are characterized by daily protein excretion of less than a gram and rarely in excess of >2gm. When >3gm category was seen, diseases such as MCD, membranous, myeloma, malignant hypertension were noted.( but all had some other clinical features). From this, a statement was made: "Thus, quantitative proteinuria in excess of 3gm becomes an excellent screening test for the diseases associated with nephrotic syndrome."
In 1980s, another paper by Ginsberg et al, proposed that use of protein/crt ratio in urine samples gave a similar comparison of patients and found >3.5gm to be the cut off for nephrotic syndrome. They studied 46 patients and found excellent correlation of 24 hour urine and spot ratio( where we get our spot ratio from).
Ref:
{kind=link}
No comments:
Post a Comment