Malignant
hypertension with AKI or AKD is a life-threatening emergency that demands rapid
blood-pressure control and carries a high risk of permanent kidney damage. When
thrombotic microangiopathy (TMA) is present, diagnostic challenges intensify.
Although complement-mediated TMA frequently presents with severe hypertension,
malignant hypertension itself can cause TMA-like vascular injury. This has been
a point of debate for many years. Does the TMA cause HTN or is HTN a cause of
TMA as well?
Early
evaluation must therefore exclude secondary hypertension and secondary TMAs,
which require etiology-specific treatment. Because a definitive distinction
between essential hypertension and complement-mediated TMA relies on genetic
testing that takes weeks, clinicians must use clinical and histologic clues to
guide early complement-blocker therapy. Significant gaps remain in
understanding pathogenesis, diagnosis, and treatment. A
recent paper in KI really takes this to a better understanding.
Early evaluation must therefore exclude secondary hypertension and secondary TMAs, which require etiology-specific treatment. Because a definitive distinction between essential hypertension and complement-mediated TMA relies on genetic testing that takes weeks, clinicians must use clinical and histologic clues to guide early complement-blocker therapy. Significant gaps remain in understanding pathogenesis, diagnosis, and treatment. A recent paper in KI really takes this to a better understanding.
Some
key messages from the review article
1. Malignant hypertension can directly cause a true TMA.
Severely elevated blood
pressure can injure small vessels, leading to endothelial damage, platelet
consumption, hemolysis, and classic TMA findings. This is not simply “secondary
hemolysis”—it is a bona fide microangiopathic process.
2. Distinguishing hypertensive TMA from other TMAs is critical.
Hypertensive TMA can mimic HUS/TTP and complement-mediated TMA.
Misdiagnosis can delay the correct therapy. The clinical context (markedly high
BP, long-standing HTN, LVH, retinal changes) is key.
3. Treatment hinges on rapid but careful blood-pressure
control.
The cornerstone is controlled BP reduction—typically in the ICU—with
parenteral antihypertensives. This alone often reverses hematologic
abnormalities and improves renal function.
4. ADAMTS13 and complement studies help guide management but should not slow
treatment.
Work-up is important, especially when features are atypical or improvement
is slower than expected. But initial management should start immediately based
on clinical suspicion.
5. Kidney recovery varies widely—follow-up matters.
Some patients experience near-complete recovery; others progress to CKD or
ESRD, especially when treatment is delayed. Long-term blood-pressure control is
essential to prevent recurrence and preserve renal function.
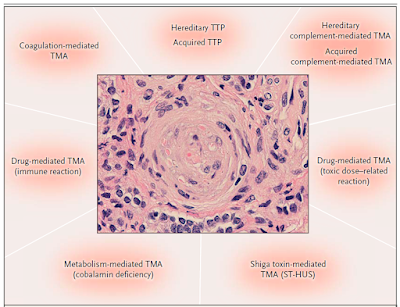
An important component is the heme component of TMA and it's presence in the systemic form of TMA. The figure( similar to the paper in KI) suggests that the complement-mediated TMA had most likely to have heme parameters of TMA as well followed by drug induced TMA and systemic diseases. HTN is not that common.

.png)