
First came the urine eosinophils-- then they were found to be useless. Apparently, despite several studies showing no clear benefit in diagnosing AIN, several folks love to order this useless test.
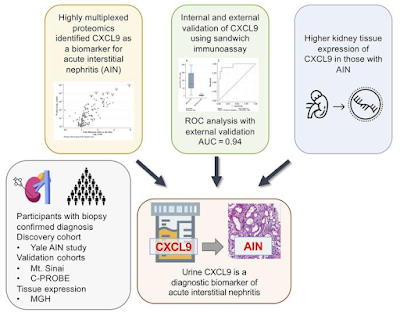
A slew of biomarkers came and went but none were real superhits for AIN. TNF-alpha and IL-9 were two potential candidates over the last few years. The authors of a recent study published in JCI performed urine proteomics to identify a potential candidate that maybe best and top contender for AIN- chemokine C-X-C motif ligand 9( CXCL9). This was then externally validated and then confirmed in kidney tissue of AIN patients compared to control groups. They also showed that urinary CXCL9 together with TNF-α and IL-9 is the optimal combination of biomarkers for AIN diagnosis.
Here is the visual abstract from the paper
What is this CXCL-9? Apparently, it is a monokine induced by IFN-γ, is a chemokine that binds to its receptor, CXCR-3, and promotes lymphocyte recruitment at sites of inflammation.
It has been shown to be associated with
acute cellular rejection( makes sense- similar to AIN)
predict future risk of rejection
AIN associated with immunotherapy ( inviting T cells and monokine)
Predicting any immune mediated events when using ICI therapy
Drawbacks-- may not tell you specifically what is the cause of the T cell invitation but can clearly tell you a clue. Urinary tests are usually challenging in oligo-anuric AIN.
It seems that the combination of TNF-alpha, CXCL-9 and IL-9 may hold promise for AIN.
Despite amazing advances in urinary markers in transplant rejection since last 15 years, we are not using it in clinical practice.
Lets hope that it is the troponin for AIN else we are still doing renal bx to confirm these tough diagnosis.