These three European Trials come as a major surprise to me.
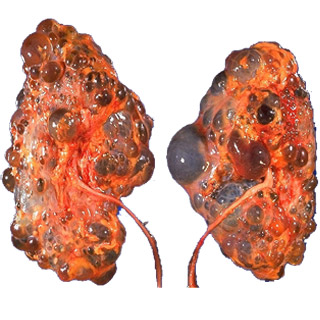
Two of them deal with the Mtor inhibitors and a clinical trial showing major disappointment in terms of decreasing GFR when used for polycystic kidney disease.
Its not the first time that the basic science data is contradicting clinical data. A nice editorial in NEJM also gives some insightful thoughts on this topic. For now, we have to await some more trails, perhaps longer term to see where we go with this drug.
Another shocker was the IDEAL trial.
This compared early initiation vs late initiation. In this study, planned early initiation of dialysis in patients with stage V chronic kidney disease was not associated with an improvement in survival or clinical outcomes.
This is an interesting study. It compared starting dialysis at 5-7ml/min vs standard practice right now and showed no difference. This goes back to the olden days when people started dialysis when patients got symptomatic rather than just a number. Perhaps we might be just going around in circles.
But some other bloggers have good comments to say.
Take a look
https://www.pediatric-nephrology.com/home/2010/06/29/233-mtoradpkd.html
https://www.pediatric-nephrology.com/home/2010/06/29/232-dialysisckdv.html
http://www.uremicfrost.com/2010/06/does-early-initiation-of-dialysis-help_27.html
http://www.uremicfrost.com/2010/06/early-vs-late-hd-initiation-video.html
http://www.uremicfrost.com/2010/06/does-early-initiation-of-dialysis-help.html
References:
http://www.ncbi.nlm.nih.gov/pubmed/20581422( IDEAL TRIAL)
http://www.ncbi.nlm.nih.gov/pubmed/20581393 ( EDITORIAL NEJM MTOR)
http://www.ncbi.nlm.nih.gov/pubmed/20581392
http://www.ncbi.nlm.nih.gov/pubmed/20581391


 The pediatric nephrology blog periodically places grand rounds that reviews news on nephrology and e-nephrology around the world. Have a look
The pediatric nephrology blog periodically places grand rounds that reviews news on nephrology and e-nephrology around the world. Have a look