Hematopoietic Stem Cell Transplant-associated thrombotic microangiopathy (TA-TMA) is a devastating complication of hematopoietic stem cell transplantation characterized by endothelial injury, microvascular thrombosis, and multiorgan dysfunction. The kidney is the most commonly and severely affected organ, with patients frequently developing acute kidney injury, proteinuria, hypertension, and long-term CKD. Renal involvement strongly predicts poor survival.
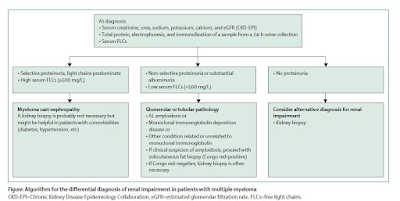
A figure from a recent review summarizes the challenges we have to diagnose TA-TMA and the limited treatment options of steroids, rituximab, and maybe eculizumab in certain cases.

Mounting evidence implicates complement dysregulation, particularly beyond the terminal C5 pathway, in TA-TMA pathogenesis. The strongest clinical data to date support narsoplimab, a monoclonal antibody targeting MASP-2 in the lectin pathway. Across multiple expanded-access and real-world case series—including the largest global cohort—narsoplimab demonstrated markedly improved 1-year survival in both adults and children, many with baseline renal dysfunction. Outcomes were best when used early, and safety signals were acceptable. These data culminated in FDA approval in December 2025 for TA-TMA in adults and children ≥2 years.
Beyond MASP-2 inhibition, upstream complement blockade is emerging. Iptacopan (factor B inhibitor) has been reported in small adult case series with improvement in hematologic markers and reduction in proteinuria, supporting a role for alternative pathway inhibition. Pegcetacoplan (C3 inhibitor) has been described in pediatric off-label cases and is under prospective investigation, reflecting interest in broader complement control for refractory disease.
Together, these studies suggest that earlier, upstream complement inhibition may provide better protection for the renal microvasculature and improve outcomes in TA-TMA compared with C5-only strategies.