An important guideline/recommendation was published in Lancet thismonth. This is an evidence based summary by the International Myeloma Working Group on myeloma related kidney disease. A must read!
Here is a summary of the findings
1.
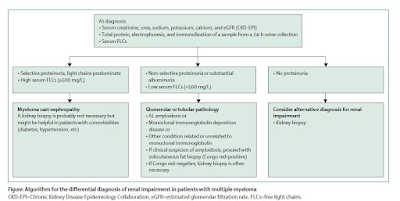
Diagnosis is important- the serum free light
chain becomes the corner stone of diagnosis. An algorithm below summarizes the
novel way of looking at it. All patients with
multiple myeloma and renal impairment should have serum creatinine, estimated
glomerular filtration rate, and FLCs measurements together with 24-h urine
total protein, electrophoresis, and immunofixation. If non-selective
proteinuria (mainly albuminuria) or involved serum FLCs value less than 500
mg/L is detected, then a renal biopsy is needed.
2.
How high is the involved FLC—can tell you if
this is cast nephropathy vs looking for a glomerular process. In addition – the
urine protein being selective vs non selective can aid in overflow proteinuria
vs a true glomerular process.
3.
Kidney biopsy is NOT required but may be
recommended if suspicious of cast nephropathy is high. Although recent studieshave shown that the IFTA and number of casts presents on renal bx can predictrenal outcomes.
4.
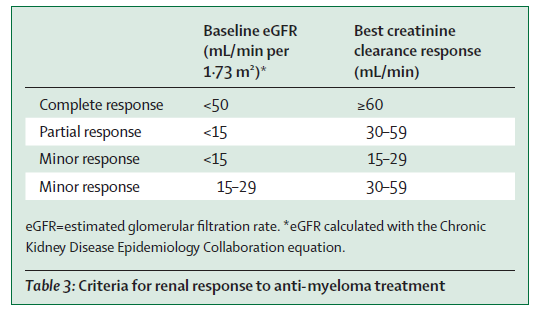
The IMWG criteria for renal response was
recommended( change in eGFR)- see table below. This is used for many studies
and validated.
5. Supportive care and high-dose dexamethasone are required for all patients with myeloma-induced renal impairment( fluids, correction of hypercalcemia, avoiding NSAIDS)
6.
Mechanical approaches do not
increase overall survival( plasma exchange- data is in the non bortezomib era,
and HCO dialyzer- two RCTs showed no benefit).
7.
Bortezomib-based regimens are
the cornerstone of the management of patients with multiple myeloma and renal
impairment at diagnosis. New quadruplet and triplet combinations, including
proteasome inhibitors, immunomodulatory drugs, and anti-CD38 monoclonal
antibodies, improve renal and survival outcomes in both newly diagnosed
patients and those with relapsed or refractory disease. The panel suggested to Start
Daratumumab + Bortezomib + Dex early and then add IMiD starting cycle two once renal
function has stabilized.
8.
Carfilzomib should not be first
line in patients with CKD as risk of TMA( first time someone mentioning this)-
glad the toxicities are being considered.. But then again- is the incidence of
TMA from carfilzomib that high- I don’t think so.
9.
Dose adjustments are discussed
for all anti Myeloma agents and their potential nephrotoxicities- mainly the
TMA from carfilzomib. There are other renal toxicities of other agents as well
not mentioned here.
10.
Conjugated antibodies, chimeric antigen receptor T-cells,
and T-cell engagers are well tolerated and effective in patients with moderate
renal impairment
11. Finally, with improved survival in myeloma, when should we consider kidney transplantation in pts. with ESKD? Should we use sustained MRD-negativity to select transplant candidates? What about the MGRS patients?—the consensus was 2 years of disease free state. But low level evidence.. I have seen sooner in most cases. Overall their outcomes are not great when compared to non myeloma ESKD.