
Linear
Staining in IF on renal pathology differential diagnosis
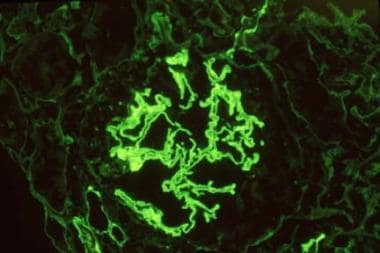
Classically the linear staining in taught in medical schools to be associated
with anti GBM disease.
On a recent discussion on ASN-Communities on this topic by many glomerular experts led to generating a differential on other causes of IF linear staining when anti GBM serologies are negative.
Dr. Richard
Glassock summarized the other causes on the forum as listed below with a few
references:
1)
Atypical anti-GBM disease- This entity recently
described by Nasr et al
in 2016 is a more indolent form of Anti GBM disease where there are no
serological markers for anti GBM and there is linear staining. It’s a slower disease
and better renal outcomes compared to classic GBM disease. The light microscopy
is variable from MPGN, TMA, to endocapillary proliferation and distinct lack of
crescents. Some cases had deposits and some didn’t. 50% of these cases have a
monoclonal disorder
2) Fibrillary GN with "pseudo-linear"
IgG deposits, often secondary to autoimmunity, infection or cancer
3) IgG4 Anti-GBM disease- most assays do not
detect IgG4 anti-GBM antibody
4) IgA1 anti-GBM disease- most assays do not detect
IgA1 anti-GBM antibody
5) Monoclonal IgG or IgA kappa directed to
COLIValpha1/2 chains
6) Wrong substrate, poor sensitivity, prozone
phenomenon in IF assays
7) "Immune sink" where all circulating
antibody is bound to GBM sites in vivo-serial testing will often resolve this
8) Spontaneous decay of circulating antibody
levels with persistence of tissue deposited antibody
9) Diabetic Nephropathy: a physico-chemical
alteration of GBM or IgG causing non-specific deposition of IgG (and albumin)
Other references
No comments:
Post a Comment